Expanding Access to Early Pancreatic Cancer Detection through ASC-Based Endoscopic Ultrasound
Summary
Pancreatic cancer remains one of the deadliest malignancies, primarily due to late diagnosis and limited access to early detection technologies. This white paper proposes how outpatient access to endoscopic ultrasound (EUS) can replicate the transformational shift that occurred when colonoscopy screening moved to ambulatory surgery centers (ASCs), fundamentally changing patient outcomes through early detection.4,5,7,8,9,12,13,17,20
The Pancreatic Cancer Crisis: A Disease Defined by Late Detection7,9
Pancreatic cancer presents one of the most challenging oncological realities in modern medicine. With an overall five-year survival rate of less than 13%, it stands as a stark reminder of what happens when cancer detection occurs too late in the disease process. The statistics become even more sobering when examining advanced disease: most patients receive their diagnosis at Stage III or IV, where five-year survival plummets to less than 3%.1,2,4,5,7,9
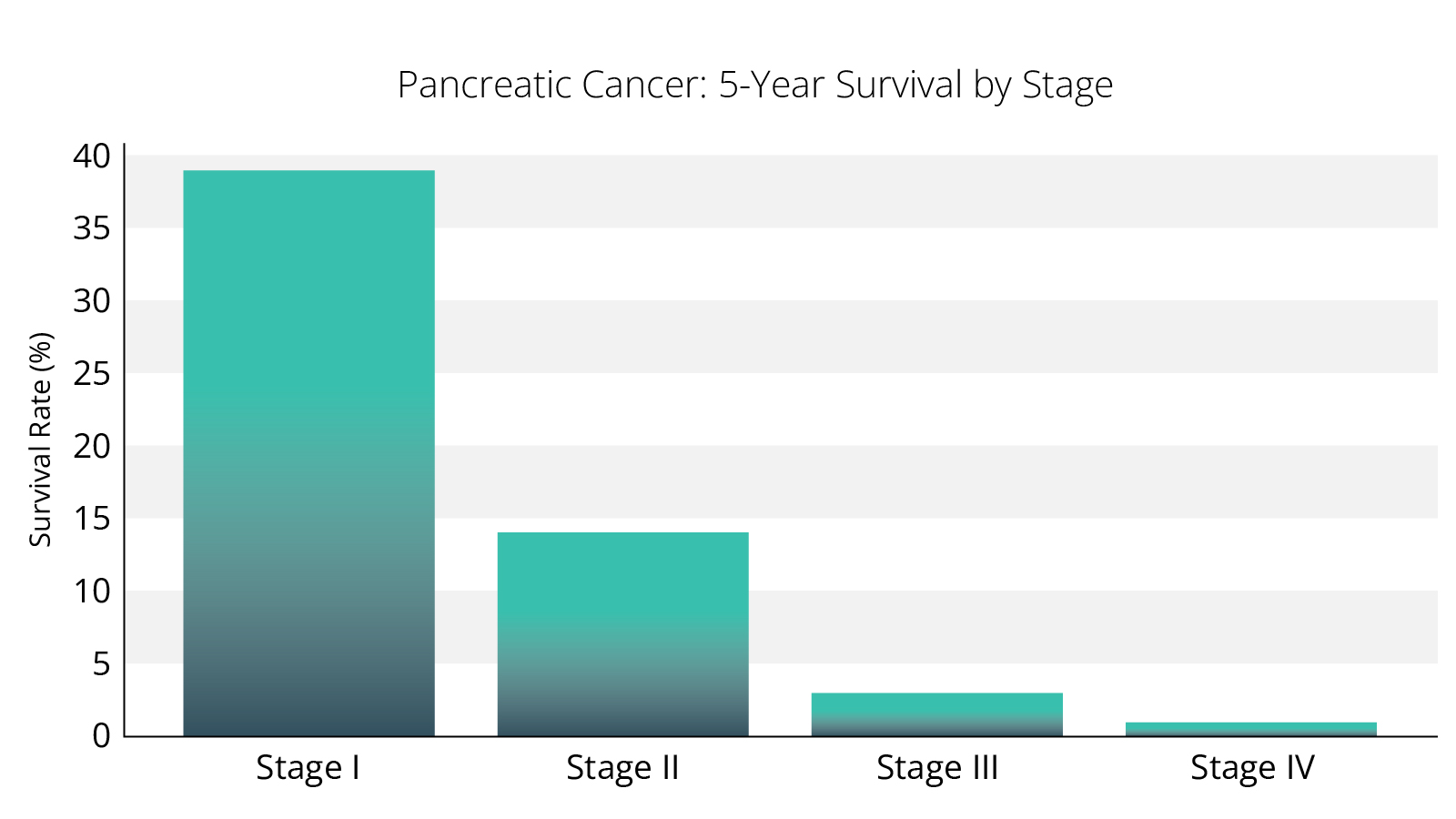 Figure 1. Pancreatic cancer survival curve — Source: SEER, ACS1,2
Figure 1. Pancreatic cancer survival curve — Source: SEER, ACS1,2
There is a common misconception that pancreatic cancer is a rapidly growing tumor. For most solid tumors a period of years elapses from the first cell gone “awry” to clinical presentation.
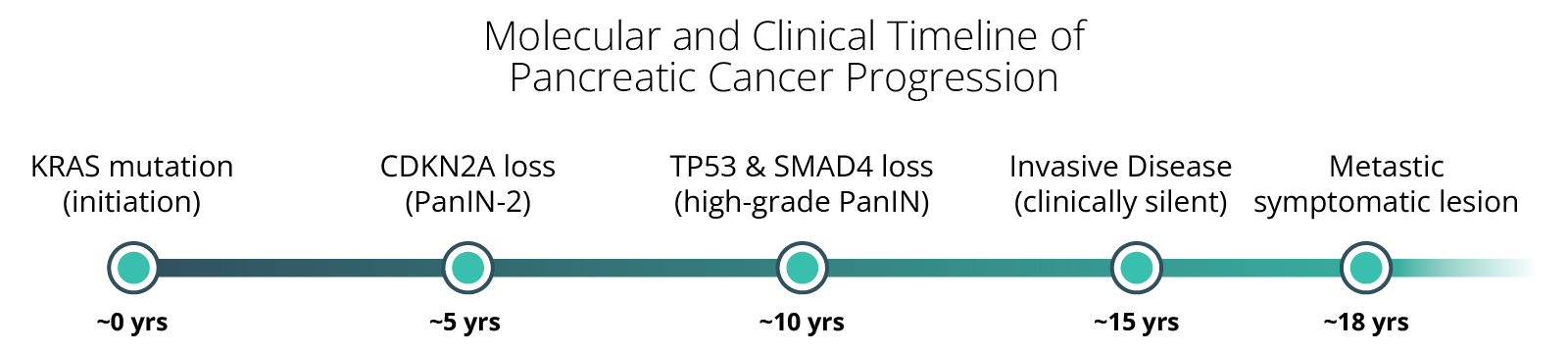
Figure 2. Timeline of pancreatic cancer initiation and progression (Yachida et al., Nature 2010)
The fundamental issue, therefore, is not the speed of progression of cancer, but rather our inability to detect it when treatment can be most effective.4,5,7,9,16
The Promise of Surveillance: Early Detection Saves Lives4,5,7,9
Pancreatic cancer meets the criteria for screening programs:
- It’s an important health problem
- There is an identifiable group of patients at risk
- There is a long “pre-clinical” phase3
- There is an accurate test (EUS) which is safe and acceptable7,8,9
- There is effective treatment for early stage disease4,5,7,9,16
- Screening is cost effective7,9
High risk individuals appropriate for screening include those with:4,5,16
- Peutz–Jeghers syndrome (STK11) → highest penetrance, strongest benefit.
- Familial pancreatic cancer kindreds (≥2 FDRs) → well-documented benefit.
- CDKN2A mutation carriers → high lifetime risk, benefit seen.
- BRCA2, PALB2, ATM with family history → moderate benefit.
- Chronic and hereditary pancreatitis (PRSS1) → benefit, but surveillance is complicated.
• New-onset diabetes in adults >50 → promising, but less validated outside research settings.
Early detection is the key to improved survival, a principle that has proven transformative across multiple cancer types while remaining elusive for pancreatic malignancies. Seventy-eight per cent of pancreatic cancers detected during surveillance programs are Stage I. The survival benefits of early-stage detection are remarkable: Stage I tumors smaller than 1 centimeter achieve up to 75% five-year survival rates, while those under 2 centimeters still maintain up to 60% five-year survival. Perhaps most significantly, surveillance-detected cancers show median survival approaching 10 years, a dramatic improvement in survival. Furthermore, from a health economics perspective, screening is considered economically feasible when the cost per Quality-Adjusted life year (QALY) is less than $50,000-100,000. At $30,000-$50,000, pancreatic cancer screening for high-risk individuals is well within the threshold.1,2,4,5,7,9,14,20
The data establishes a clear principle: early detection of pancreatic cancer is beneficial and potentially curative. The challenge lies not in proving the value of early detection, but in making it accessible to those who need it most. That has been the missing element.4,5,7,9
Endoscopic Ultrasound: The Superior Detection Technology7,8,9
Endoscopic ultrasound represents the gold standard for detecting small pancreatic lesions, consistently outperforming both CT and MRI in identifying sub-centimeter abnormalities (Figure 3).4 Beyond its superior imaging capabilities, EUS serves as a comprehensive diagnostic tool that can identify critical risk factors in the general population, including pancreatic cysts, intraductal papillary mucinous neoplasms (IPMN), chronic pancreatitis, and fatty pancreas changes.7,8,9,15
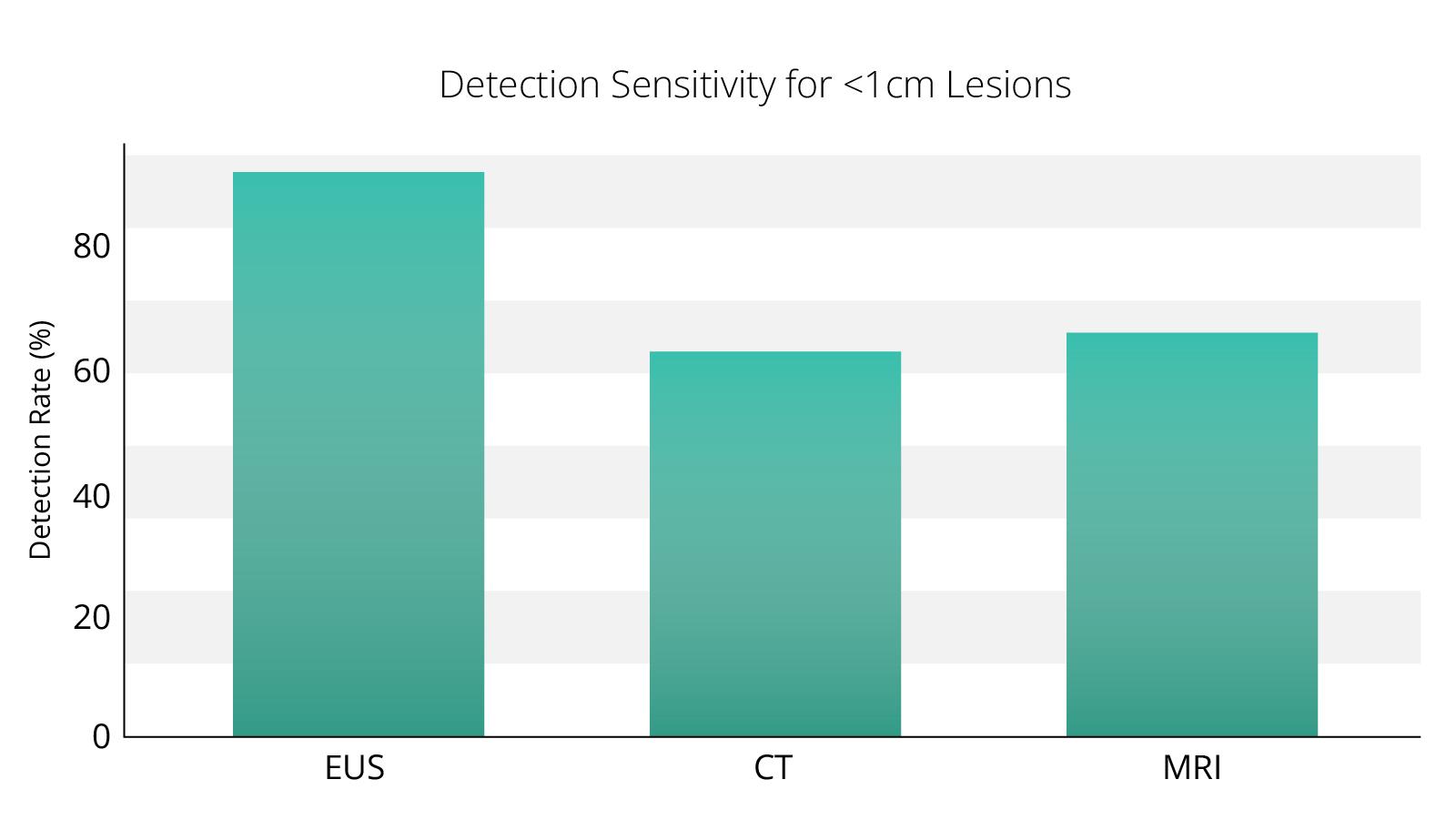 Figure 3. Detection sensitivity of different modalities4
Figure 3. Detection sensitivity of different modalities4
EUS technology is also future proof. As emerging blood tests raise the possibility of pancreatic cancer detection, EUS will remain the essential modality for confirmation and precise characterization of lesions.7,8,9,20
The parallels to colorectal cancer screening are instructive: Colonoscopy screening has cut colorectal cancer incidence nearly in half since the 1980s and raised five-year survival from 50% to 65%, with 89% survival at early stages versus 16% late. Long-term studies show up to 25% lower incidence in screened groups, and shifting procedures to ASCs has made this success more accessible and cost-effective.1,2,7,9,12,13,17,20
Colonoscopy screening has been successful because it meets three critical criteria. High-risk groups are clearly identifiable, including adults over 50 and those with specific risk factors. The test itself is impactful, (the ability to remove precancerous polyps and detect early cancers). Most importantly, the screening modality, colonoscopy became accessible through widespread deployment in outpatient settings.7,9,12,13,17
EUS meets the first two screening criteria perfectly. Early detection of small pancreatic lesions demonstrably saves lives, and high-risk groups are increasingly well-defined through advances in genetic testing and risk stratification. For these reasons, multiple consensus guidelines (CAPS Consortium, AGA, NCCN, ASGE, ESGE) recommend screening of high-risk individuals as the Standard of Care. The critical obstacle remains access.4,5,7,8,9,20
The Access Problem: Infrastructure and Cost Barriers7,9
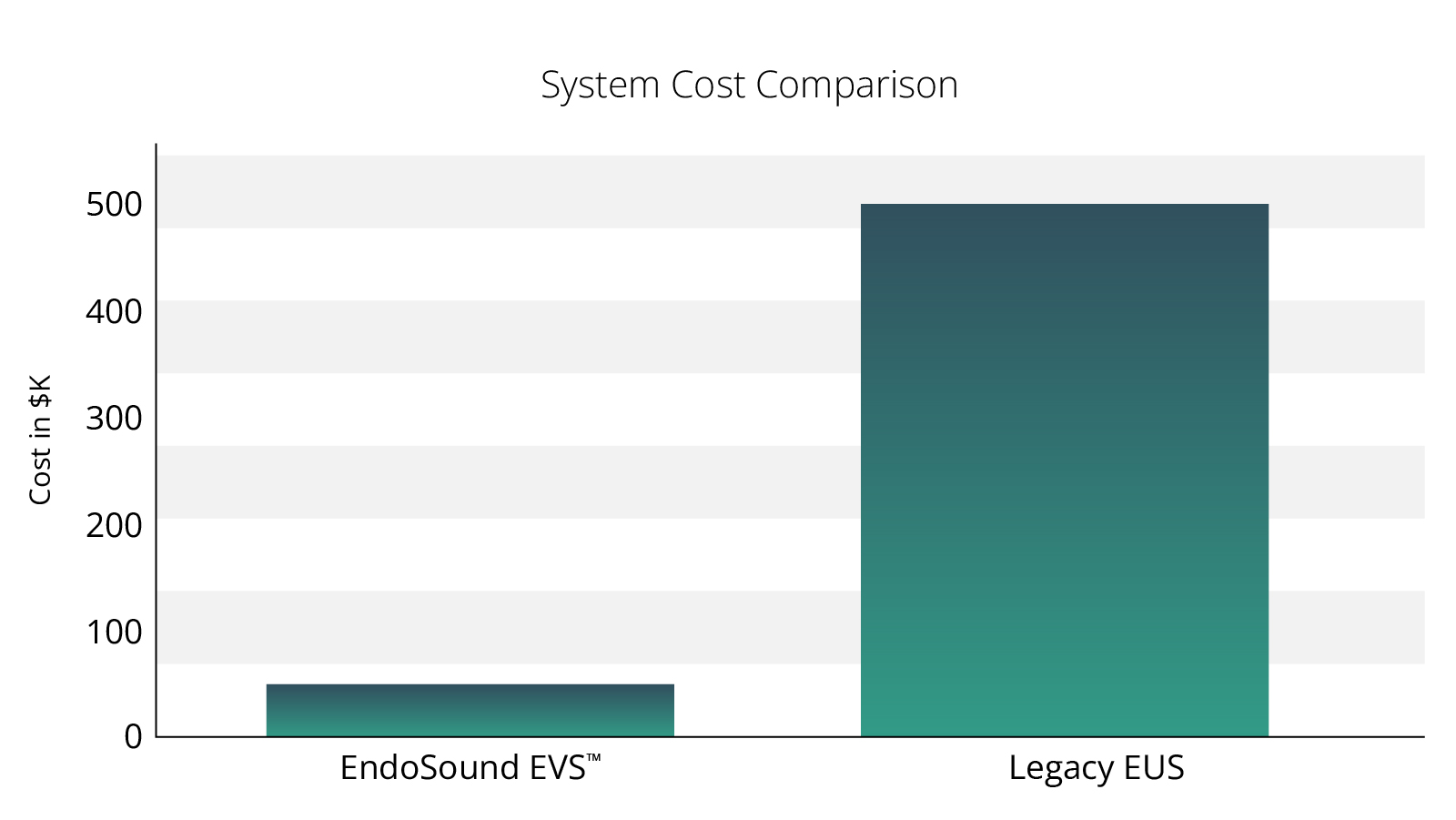
The current deployment model for EUS technology creates fundamental barriers to widespread screening implementation. Legacy EUS systems cost more than $500,000, representing a significant capital investment that limits deployment primarily to large hospital systems. As it was for colonoscopy, a hospital-based model represents the worst possible setting for accessible screening programs, creating geographic, scheduling, and cost barriers that prevent routine surveillance of high-risk populations.7,8,9,12,13,17,18
The contrast with colonoscopy is stark. Colonoscopy’s migration to ASCs revolutionized colorectal cancer screening by making the procedure more accessible, cost-effective, and patient-friendly. The ASCs have proven their ability to deliver high-quality endoscopic procedures while reducing costs and improving convenience for patients.7,9,12,13,17
The Solution: EndoSound Vision System™ Technology
The EndoSound Vision System (EVS™) technology addresses the fundamental access barriers that have limited EUS deployment for pancreatic cancer screening. At a fraction of the capital cost of legacy systems, EVS makes EUS technology economically viable for ASCs and smaller healthcare facilities. The system’s compatibility with existing Olympus, Pentax, and Fujifilm endoscopes demonstrates its value by using the center’s existing endoscopes, further reducing implementation barriers.7,8,9,12,13,17,18,19
The portable and scalable design of EVS enables flexible deployment models that can adapt to different healthcare settings and patient populations. The disposable-based model ensures consistent quality, making it ideal for high-volume screening applications. Importantly, the technology is fully reimbursed through existing CMS EUS codes and further subsidized via C-code C1606 (Transition Pass Through payment), creating an economically sustainable model for widespread deployment.7,8,9,18,19,20
The EVS represents the ideal technology partner for ASC deployment and has significant potential for global health applications where traditional EUS systems are economically unfeasible. The combination of clinical effectiveness, economic efficiency, and operational simplicity creates the conditions necessary for transformational change in early detection of pancreatic cancer.4,5,7,8,9,18,19
Conclusions
The opportunity to replicate colonoscopy’s transformational impact on cancer outcomes now exists for pancreatic cancer through EUS technology deployed in ASCs. This represents not an aspirational goal but an operational reality that can be implemented immediately with existing technology and infrastructure.7,8,9,12,13,17
The clinical evidence supporting EUS-based early detection is robust and growing.4,5,6,7,9,10,17 The economic model for ASC-based deployment shows sustainability and promise.21,22,23 The technology platform through EVS is clinically validated, economically efficient, and immediately deployable. The convergence of these factors creates an unprecedented opportunity to change the outcome curve for one of the world’s deadliest cancers.4,5,7,8,9,18,19,20
The question is no longer whether early detection can improve pancreatic cancer outcomes, but rather how quickly we can scale access to make these benefits available to the patients who need them most. Just as colonoscopy moved into ASCs and saved countless lives through early detection, the same transformation can now be achieved for pancreatic cancer through the strategic deployment of EUS technology in outpatient settings.4,5,7,8,9,12,13,17,20
References (Grouped)
Epidemiology and Survival
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1):7–33.
2. SEER Cancer Statistics Review, 1975–2020. National Cancer Institute, Bethesda, MD.
3. Yachida S, Jones S, Bozic I, et al. Distant metastasis occurs late during the genetic evolution of pancreatic cancer. Nature. 2010;467(7319):1114–1117.
Screening Criteria and Guidelines
4. Canto MI, Almario JA, Schulick RD, et al. Risk of neoplastic progression in high-risk individuals under surveillance. JAMA Oncol. 2023;9(7):1001–1009.
5. Lennon AM, Wolfgang CL, Canto MI, et al. Pancreatic cancer surveillance in high-risk individuals: the CAPS5 study. J Clin Oncol. 2022;40(34):3888–3897.
6. Wilson JMG, Jungner G. Principles and practice of screening for disease. World Health Organization. 1968.
7. Dumonceau JM, Deprez PH, Jenssen C, et al. ESGE Clinical Guideline. Endoscopy. 2017;49(7):695–714.
16. NCCN Clinical Practice Guidelines in Oncology: Pancreatic Adenocarcinoma. Version 2.2024.
EUS Accuracy and Performance
8. Simons-Linares CR, Wander P, Vargo J, Chahal P. Endoscopic ultrasonography: an inside view. Cleve Clin J Med. 2020;87(3):175–183.
9. Saftoiu A, Vilmann P. Endoscopic ultrasound for early detection of pancreatic cancer. Endosc Ultrasound. 2016;5(3):163–169.
10. Uchida D, Kato H, Matsumoto K, et al. Single-session esophagogastroduodenoscopy and endoscopic ultrasound for pancreaticobiliary screening. BMC Gastroenterol. 2019;19:220.
11. Jung Y, et al. Endosonography for right-sided and acute upper intestinal misery (EFRAIM): a prospective study. Endoscopy. 2013;45(5):381–386.
15. Petrov MS. Fatty change of the pancreas: the Pandora’s box of pancreatology. Lancet Gastroenterol Hepatol. 2023;8(5):427–439.
Colonoscopy Model
12. Zauber AG. The Impact of Screening on Colorectal Cancer Mortality and Incidence. Dig Dis Sci. 2015;60(3):681–691.
13. American Cancer Society. Cancer Facts & Figures 2024. American Cancer Society; 2024.
Cost-Effectiveness & ASC Economics
14. Neumann PJ, Cohen JT, Weinstein MC. Updating cost-effectiveness—the curious resilience of the $50,000-per-QALY threshold. N Engl J Med. 2014;371:796–797.
17. Mehta PP, et al. Ambulatory surgical centers and their role in endoscopy. Gastrointest Endosc Clin N Am. 2015;25(2):307–318.
18. EndoSound internal market research, 2024 (regarding EUS capital cost structures).
19. EndoSound Coding Guide, 2025 (CMS EUS codes and C1606).
20. Lin C-Y, et al. Advances in early pancreatic cancer detection: imaging, biomarkers, and AI. Biomedicines. 2025;13(7):1733.
21. Valencia, Brenda AGTS; Sachdev, Mankanwal MD; Bradley, Debi MSN-L RN; Das, Ananya MD, FACG. Safety and Economic Feasibility of Endoscopic Ultrasonography (EUS) in a Free-Standing Ambulatory Surgery Center (ASC) Is Comparable to Colonoscopy: 1932. American Journal of Gastroenterology. 109():p S571, October 2014.]
22. Neil Sharma, MD “Performing Outpatient EUS in the Ambulatory Setting. Is it a worthwhile Endeavor?” https://www.youtube.com/watch?v=WN_oKUIp8jQ; FLORIDA LIVE EUS 2025.
23. Stuart Akerman and Stephen Steinberg, Preliminary Results of Utilizing A Novel EUS Solution in an ASC Setting, American College of Gastroenterology Poster session, 2024
